The brachial plexus is a network of nerve fibers, running from the spine, formed by the ventral rami of the lower four cervical and first thoracic nerve roots (C5-C8, T1). It proceeds through the neck, the axilla
(armpit region), and into the arm. It is a network of nerves passing
through the cervico-axillary canal to reach axilla and innervates
brachium (upper arm), antebrachium (forearm) and hand
Lesions can lead to severe functional impairment.[1]
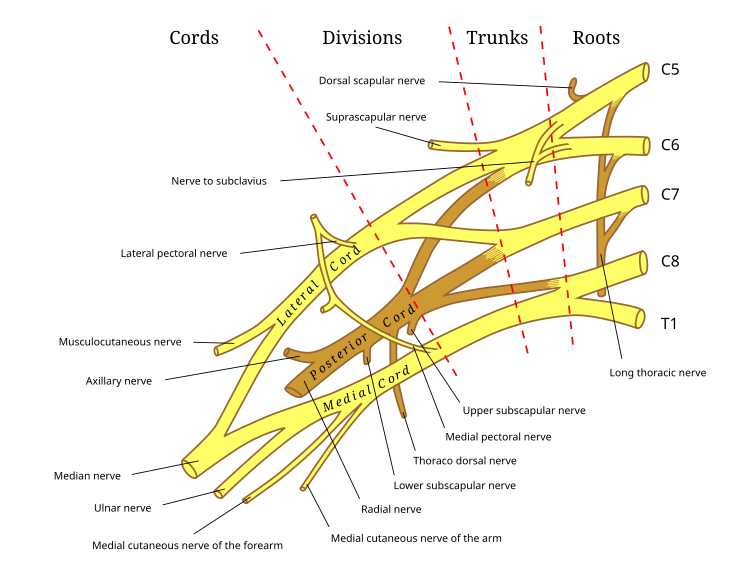
 Anatomical illustration
of the brachial plexus with areas of roots, trunks, divisions and cords
marked. Clicking on names of branches will link to their Wikipedia
entry.
Anatomical illustration
of the brachial plexus with areas of roots, trunks, divisions and cords
marked. Clicking on names of branches will link to their Wikipedia
entry.
 Diagrammatic representation of the brachial plexus using colour to
illustrate the contributions of each nerve root to the branches
Diagrammatic representation of the brachial plexus using colour to
illustrate the contributions of each nerve root to the branches
Some mnemonics for remembering the branches:
Acute brachial plexus neuritis is a neurological disorder that is characterized by the onset of severe pain in the shoulder region. Additionally, the compression of cords can cause pain radiating down the arm, numbness, paresthesia, erythema, and weakness of the hands. This kind of injury is common for people who have prolonged hyperabduction of the arm when they are performing tasks above their head.
Function
The brachial plexus is responsible for cutaneous and muscular innervation of the entire upper limb, with two exceptions: the trapezius muscle innervated by the spinal accessory nerve (CN XI) and an area of skin near the axilla innervated by the intercostobrachial nerve.Lesions can lead to severe functional impairment.[1]
Anatomy
The brachial plexus is divided into Roots, Trunks, Divisions, Cords, and Branches. There are five "terminal" branches and numerous other "pre-terminal" or "collateral" branches that leave the plexus at various points along its length.Root
The five roots are the five anterior rami of the spinal nerves, after they have given off their segmental supply to the muscles of the neck. The brachial plexus emerges at five different levels; C5, C6, C7, C8, and T1. There is prefixed or postfixed formations in some cases which involves c4 or T2 respectively .Trunk
These roots merge to form three trunks:Division
Each trunk then splits in two, to form six divisions:- anterior divisions of the upper, middle, and lower trunks
- posterior divisions of the upper, middle, and lower trunks
Cord
These six divisions will regroup to become the three cords. The cords are named by their position with respect to the axillary artery.- The posterior cord is formed from the three posterior divisions of the trunks (C5-C8,T1)
- The lateral cord is the anterior divisions from the upper and middle trunks (C5-C7)
- The medial cord is simply a continuation of the anterior division of the lower trunk (C8,T1)
Branches
The branches are listed below. Most branch from the cords, but a few branch (indicated in italics) directly from earlier structures. The five on the left are considered "terminal branches".Diagram

Specific branches
Bold indicates primary spinal root component of nerve. Italics indicate spinal roots that frequently, but not always, contribute to the nerve.| From | Nerve | Roots[2] | Muscles | Cutaneous |
| roots | dorsal scapular nerve | C4, C5 | rhomboid muscles and levator scapulae | - |
| roots | long thoracic nerve | C5, C6, C7 | serratus anterior | - |
| roots | branch to phrenic nerve | C5 | Diaphragm | - |
| upper trunk | nerve to the subclavius | C5, C6 | subclavius muscle | - |
| upper trunk | suprascapular nerve | C5, C6 | supraspinatus and infraspinatus | - |
| lateral cord | lateral pectoral nerve | C5, C6, C7 | pectoralis major and pectoralis minor (by communicating with the medial pectoral nerve) | - |
| lateral cord | musculocutaneous nerve | C5, C6, C7 | coracobrachialis, brachialis and biceps brachii | becomes the lateral cutaneous nerve of the forearm |
| lateral cord | lateral root of the median nerve | C5, C6, C7 | fibres to the median nerve | - |
| posterior cord | upper subscapular nerve | C5, C6 | subscapularis (upper part) | - |
| posterior cord | thoracodorsal nerve (middle subscapular nerve) | C6, C7, C8 | latissimus dorsi | - |
| posterior cord | lower subscapular nerve | C5, C6 | subscapularis (lower part ) and teres major | - |
| posterior cord | axillary nerve | C5, C6 | anterior branch: deltoid and a small area of overlying skin posterior branch: teres minor and deltoid muscles |
posterior branch becomes upper lateral cutaneous nerve of the arm |
| posterior cord | radial nerve | C5, C6, C7, C8, T1 | triceps brachii, supinator, anconeus, the extensor muscles of the forearm, and brachioradialis | skin of the posterior arm as the posterior cutaneous nerve of the arm |
| medial cord | medial pectoral nerve | C8, T1 | pectoralis major and pectoralis minor | - |
| medial cord | medial root of the median nerve | C8, T1 | fibres to the median nerve | portions of hand not served by ulnar or radial |
| medial cord | medial cutaneous nerve of the arm | C8, T1 | - | front and medial skin of the arm |
| medial cord | medial cutaneous nerve of the forearm | C8, T1 | - | medial skin of the forearm |
| medial cord | ulnar nerve | C8, T1 | flexor carpi ulnaris, the medial two bellies of flexor digitorum profundus, the intrinsic hand muscles except the thenar muscles and the two most lateral lumbricals | the skin of the medial side of the hand and medial one and a half fingers on the palmar side and medial two and a half fingers on the dorsal side |
- Posterior cord branches
- STAR - subscapular (upper and lower), thoracodorsal, axillary, radial
- RATS- Radial nerve, Axillary nerve, Thoracodorsal nerve, Subscapular (Upper & Lower)nerve.
- ULTRA - upper subscapular, lower subscapular, thoracodorsal, radial, axillary
- ULNAR- Upper subscapular nerve, Lower subscapular nerve,Nerve to latissimus dorsi, Axillary nerve, Radial nerve.
- Lateral Cord Branches
- LLM "Lucy Loves Me" - lateral pectoral, lateral root of the median nerve, musculocutaneous
- Love Me Latha (LML) - Lateral pectoral nerve, Musculocutaneous nerve, Lateral root of Median Nerve.
- Look My Lancer-Lateral pectoral nerve, Musculocutaneous nerve,Lateral root of Median nerve.
- Medial Cord Branches
- MMMUM "Most Medical Men Use Morphine" - medial pectoral, medial cutaneous nerve of arm, medial cutaneous nerve of forearm, ulnar, medial root of the median nerve
- Union of 4 Medials - Ulnar nerve, Medial cutaneous nerve of arm, Medial cutaneous nerve of forearm, Medial pectoral nerve, Medial root of Median Nerve.
- 5 main nerves of brachial plexus, in order laterally to medially
- "My Aunty Recognised My Uncle" - Musculocutaneous, axillary, radial, median, ulnar.
Injuries
Brachial plexus injury affects cutaneous sensations and movements in the upper limb. They can be caused by stretching, diseases, and wounds to the lateral cervical region (posterior triangle) of the neck or the axilla. Depending on the location of the injury, the signs and symptoms can range from complete paralysis to anesthesia. Testing the patient's ability to perform movements and comparing it to their normal side is a method to assess the degree of paralysis. A common brachial plexus injury is from a hard landing where the shoulder widely separates from the neck (such as in the case of motorcycle accidents or falling from a tree). These stretches can cause ruptures to the superior portions of the brachial plexus or avulse the roots from the spinal cord. Upper brachial plexus injuries are frequent in newborns when excessive stretching of the neck occurs during delivery. Studies have shown a relationship between birth weight and brachial plexus injuries; however, the number of cesarean deliveries necessary to prevent a single injury is high at most birth weights.[3] For the upper brachial plexus injuries, paralysis occurs in those muscles supplied by C5 and C6 like the deltoid, biceps, brachialis, and brachioradialis. A loss of sensation in the lateral aspect of the upper limb is also common with such injuries. An inferior brachial plexus injury is far less common, but can occur when a person grasps something to break a fall or a baby's upper limb is pulled excessively during delivery. In this case, the short muscles of the hand would be affected and cause the inability to form a full fist position.[4] In order to differentiate between a pre ganglionic and a post ganglionic type of injury on clinical examination one has to keep the following points in mind. In pre ganglionic injuries there will be loss of sensation above the level of clavicle, presence of pain in an otherwise insensate hand, presence of ipsilateral Horner's syndrome and loss of function of muscles supplied by branches arising directly from roots i.e. long thoracic nerve palsy leading to winging of scapula and elevation of ipsilateral diaphragm due to phrenic nerve palsy.Acute brachial plexus neuritis is a neurological disorder that is characterized by the onset of severe pain in the shoulder region. Additionally, the compression of cords can cause pain radiating down the arm, numbness, paresthesia, erythema, and weakness of the hands. This kind of injury is common for people who have prolonged hyperabduction of the arm when they are performing tasks above their head.
No comments:
Post a Comment